Research
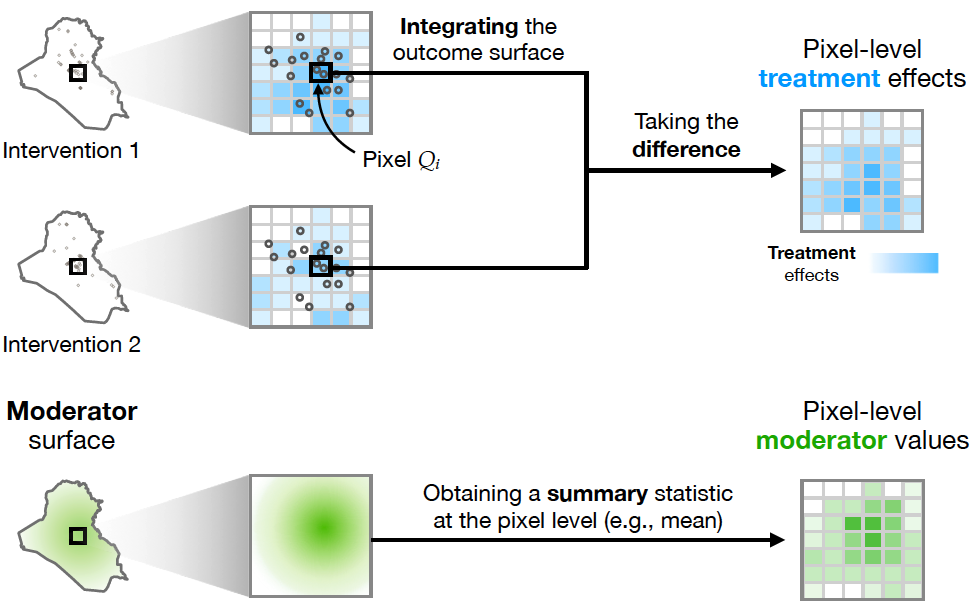
Spatiotemporal causal inference with arbitrary spillover & carryover effects
A desire to demonstrate resolve motivates insurgent attacks more than revenge or grievance in Iraq.
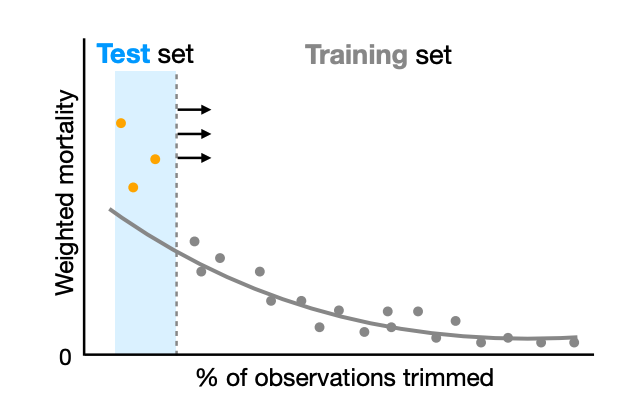
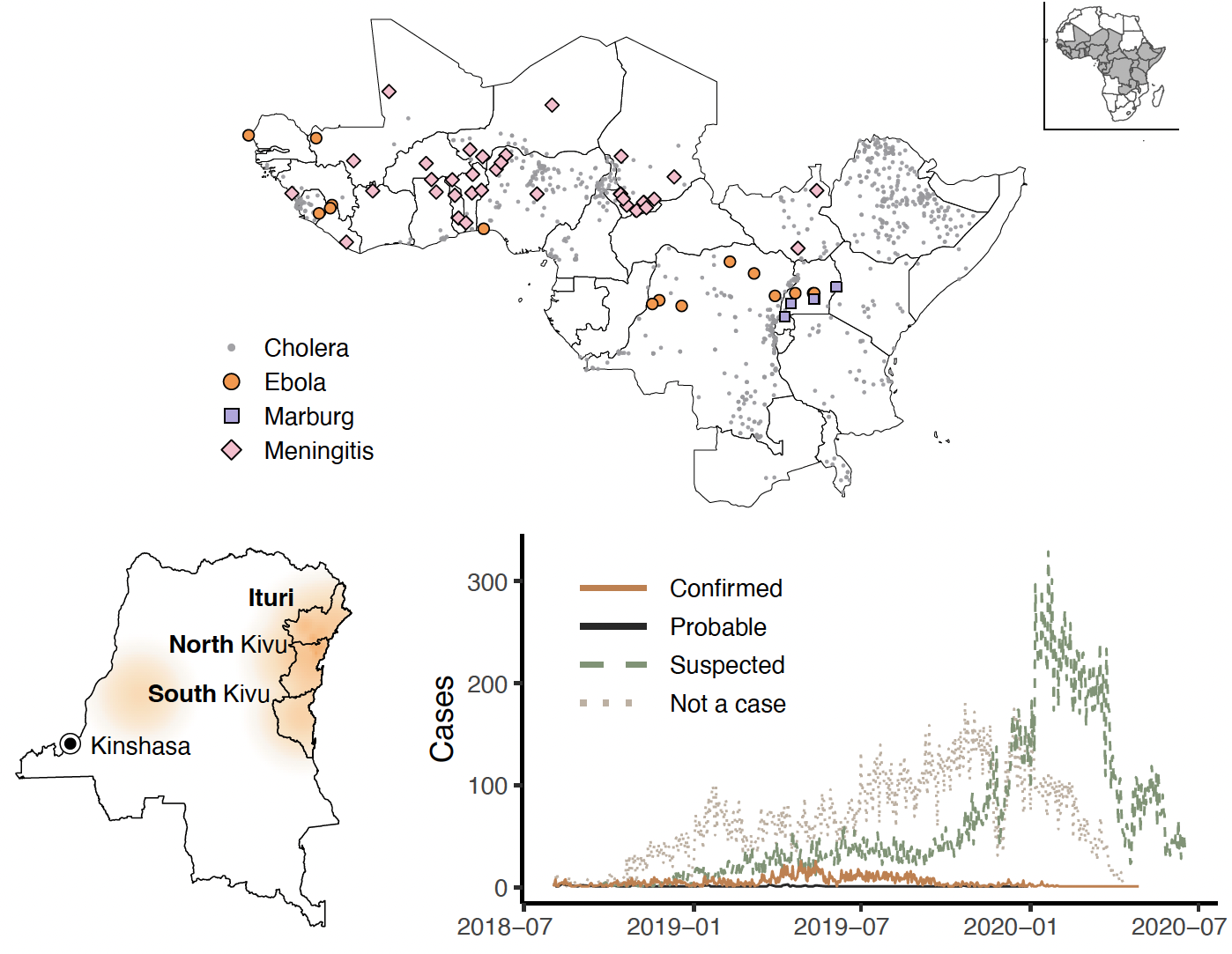
Survey estimates of wartime mortality
Accounting for political and strategic incentives in surveys produces more accurate estimates of wartime mortality.
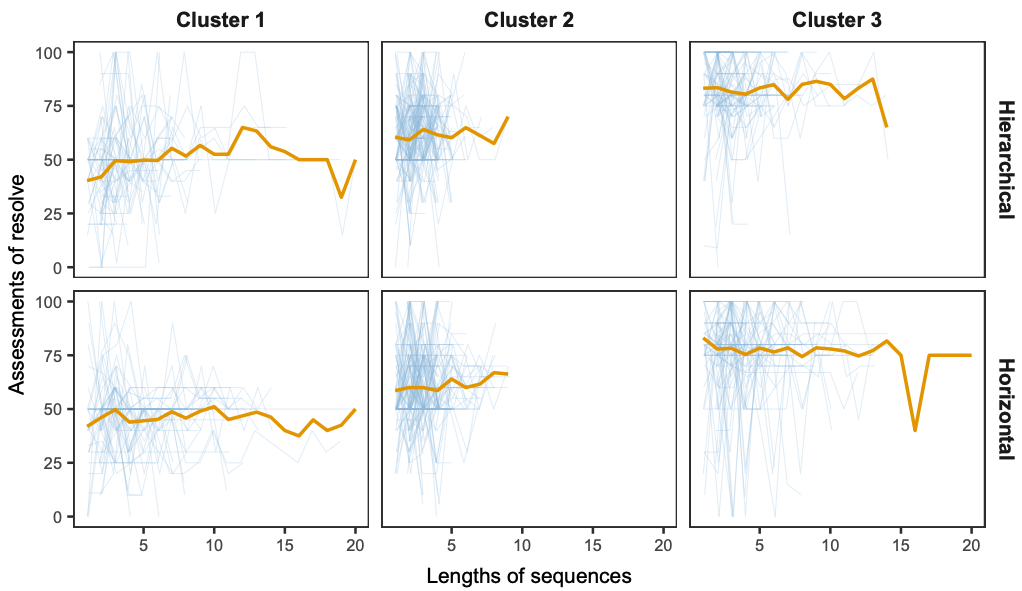
Diplomacy by committee
In diplomacy, groups rely more on first impressions and update less from signals than individuals.



